Frequently Asked Questions
Check out our FAQ, or search for information here:
How do I become a Caring Dads Facilitator?
Caring Dads is a trademarked intervention program that is run exclusively by accredited Facilitators, in good standing, and according to our published program guidelines.
Accredited Caring Dads Facilitators have completed Caring Dads facilitator training and are either employed by a social service provider or a registered mental health professional (e.g., registered social workers, psychologists, psychotherapists) or unless otherwise agreed to by Caring Dads.
Facilitator Training events are available in virtual and in-person formats. Course tuition includes facilitator traning, 4 clinical consultation sessions, Caring Dads program manual, and ongoing access to the Caring Dads Provider Portal. Accreditation is a one-time process.
How can I get more people interested in referring men to Caring Dads?
For Caring Dads, as with all other programs newly introduced to a community, enthusiasm for offering a program initially outstrips referral to the program. In the case of service to abusive fathers, this problem with start-up is exacerbated by traditional bias in child protection towards working with mothers and children and excluding fathers. There are numerous ways to overcome these challenges, and within a year or two of beginning to offer the Caring Dads program, difficulties with getting referral will be supplanted with difficulties stemming referral. For those early days, however, the following tips are useful.
Ensure community support. As has already been emphasized in this manual, community support is essential to offering the Caring Dads program. With community support, difficulties with referral can be problem-solved as a group with key referral agents sitting together with those offering the Caring Dads program. Subpoena or recruit a champion for Caring Dads from within major referral agencies. It has been our experience that appreciation of the need to engage abusive fathers by management of an agency often outpaces shifts in the frontline practices of father engagement.
One strategy that we have found very helpful for closing this gap is to set aside paid time for someone from within major referral agencies (i.e., child protection, probation, child and family mental health) to champion referral to Caring Dads. Jobs of this champion typically include spreading the word about the availability of Caring Dads within the agency (e.g., making announcement at team meetings), reviewing open cases to identify and promote likely referrals to Caring Dads, providing direct support to frontline staff in making their first few referrals (e.g., modeling a discussion with fathers about the need for service), and acting as a liaison between the referral agency and Caring Dads for communication and problem-solving. Continually encourage service providers from across sections to consider fathers in their risk assessment and case planning.
A third strategy for promoting referral to Caring Dads is to continue to spread the word about the need to include fathers in conceptualizations of children’s safety and well-being. There are multiple initiatives in child protection, child and family mental health and in probation to better consider men’s role as fathers. Those in the Caring Dads program should contribute to and support these efforts whenever possible. Spread stories of success. One of the reasons that referral to Caring Dads grows is that people get to know about success. Offer opportunities for cross-training. Finally, we have had considerable success in promoting referral to Caring Dads by opening options for cross-agency co-facilitation of groups. There is currently a great need for training in how to work with men in general, and with fathers specifically. One way for practitioners to increase their skills working with men is to get experience offering Caring Dads. When a Caring Dads group is offered by a co-facilitation team from across two different agencies, there is an automatic connection to two different referral sources.
Which fathers are eligible for attending a Caring Dads program?
The specific details of eligibility to Caring Dads vary by community due to the differing regulations, relationships and practices. In general, we recommend the following eligibility criteria be met:
A. Identification of concerns about abusive or neglectful parenting or exposure of children to domestic violence.
The Caring Dads program was designed to meet the needs of fathers who are abusive in their families. It was not designed for fathers who needed more general parenting support. The following are examples of times fathers would be eligible:
○ Have physically and emotionally abused their children
○ Are at risk of maltreating their children
○ Have an over-bearing, controlling style of interacting with their children
○ Alternatively involved and distant with their children
○ Have physically or emotionally abused children’s mothers
○ Have separated from their partners yet continue to be in frequent hostile conflict with their children’s mothers
○ Have abandoned one or more child and moved onto another family and are at-risk of abusing or abandoning other children
B. Have contact with at least one child
The Caring Dads program requires that men have some contact with their children. Contact can be supervised and can be minimal (e.g. 1 hour a week). Contact is necessary for men to apply lessons learned in group and for facilitators to gather a sense of the degree of change. Homework exercises involve practicing more child-centered fathering and reporting on both positive and problematic father-child interactions.
C. Are referred by someone who can follow-up on men’s progress
Because Caring Dads aims to reduce risk to children, it is critically important to consider steps that might be taken if fathers fail to make progress, show continued abusive behavior or continue to exposure their children to abuse of their mothers. Men must therefore be referred by someone who is intending to remain connected to at least one member of the family for the duration of the program. Often, men are referred by child protection or probation workers, though we also take referrals from child mental health services or other organizations as long as they understand and are willing to collaborate in meeting the goal of ensuring child safety and well-being.
D. Able to comply with intake process
Finally, to be eligible to begin intervention, men need to be able to comply with the intake process which includes attending an intake meeting, completing intake forms and showing a willingness to discuss his situation. In cases where men who repeatedly fail to attend scheduled intakes and/or who are unwilling to participate in the intake process, serious concerns should be conveyed to the referral agent about potentially elevated level of risk and clear consequences should be applied.
Men referred to Caring Dads have a range of other co-morbid problems as well. Most of the time, other challenges do not present a barrier to involvement in Caring Dads. Exceptions are as follows:
○ Legal termination of parental rights has been initiated or is currently intended, or fathers are in the midst of a family court dispute over custody of children that might result in loss of father-child contact. There are two legal situations that lead us to be reticent about accepting men into Caring Dads. The first is where child protection is initiating or activity considering legal action that would terminate fathers’ contact with their children. The second is cases where fathers are at a critical point in a custody and access dispute (e.g. he will hear in three weeks if he can have any access). Fathers in both of these situations are at-risk of having their contact with their children terminated and, since they are in the midst of a crisis, are unlikely to be able to devote the necessary psychological resources to creating change in their family relationships.
○ Severe alcohol and/or substance misuse. Group members must be clean and sober to attend the program. Men who have not addressed their substance and alcohol misuse and not likely to be able to participate in a meaningful fashion. Those men who are actively engaged in treatment or who can maintain abstinence on the day of the group may be considered appropriate.
○ Low risk fathers who would benefit from supportive intervention. Due to a lack of fathering intervention available in some communities, Caring Dads occasionally gets requests for service from low-risk fathers who need supportive intervention (e.g., peer support around parenting, tips and strategies). Fathers at low-risk for abuse, who have with strong positive connections with their children and respectful cooperative relationships with their children’s mothers are not appropriate referrals to Caring Dads.
○ Literacy and language issues. Assistance should be given to men with literacy problems to participate on the group although occasionally some men’s cognitive functioning may be at a level that means this intervention will not be appropriate.
○ Sexual abuse of children. There are important differences in the characteristics and offence cycles of fathers who have sexually abused their children as compared to fathers who have perpetrated physical abuse, emotional abuse, neglect or exposed their children to abuse of their mother. Caring Dads was not designed to meet the needs of men with a history of sexually abusing children, and these men will not generally benefit from this program. Sexually abusive men are better serviced with treatment specifically designed to identify, monitor and change cycles of sexual offending. Men who have perpetrated sexual abuse and who have completed treatment, and who are now of concern due to physical or emotional abuse, neglect or abuse of children or of children’s mothers may be appropriate referrals. Decisions in this situation will need to be made on a case by case basis, considering men’s history and pattern of sexually offending against children.
Can mothers attend Caring Dads programs?
We have decided to focus our intervention efforts on fathers alone because there is a general lack of parenting programs available to men. It is our belief that fathers can and often do play a very important role in their children's development and that programs should be available to help men improve their parenting.
Why is the Caring Dads program 17 weeks long?
The decision to run for 17 weeks represents our best comprise on covering necessary material and respecting cost restraints. Subsequently published meta-analysis of the literature on parent interventions for populations at-risk for abuse and reviews of fatherhood programs are consistent in concluding that treatments lasting a minimum of three months are associated with greater gains than shorter ones (Bronte-Tinkew et al., 2007, Lundahl et al., 2006).
Do you offer separate programs for partner vs child abusing fathers?
We are sometimes asked about offering, or developing, separate Caring Dads groups for men who have maltreated their children and those who have exposed their children to abuse of their mothers. The reality is that there is considerable overlap between men’s perpetration of domestic violence and both their physical abuse and neglect of children. Edleson’s (1999) review of the literature concluded that there is a 30 to 60% overlap of domestic violence and child physical abuse perpetration; a range that has been confirmed in subsequent reviews (e.g., Jouriles, McDonald, Slep, Heyman & Garrido, 2008) and on the basis of nationally representative samples (e.g., Hamby, Finkelhor, Turner & Ormrod, 2010). In our clinical samples of men, the degree of overlap is even higher with as many as three quarters of Caring Dads fathers having problems with both their relationships with their partners and with their relationships with their children (Scott et al., 2007). Given the overlap in these two presenting issues, we recommend that fathers who have maltreated their children and those who have exposed their children to domestic violence be treated together.
How does Caring Dads work with other intervention programs?
There is ongoing debate in the field on the best time to offer Caring Dads to men who have abused women, and more generally, on the relationship between Caring Dads and programs for partner abusive men. Given the complexity of situations presented by men, women and children, we recommend against blanket restrictions (e.g. Caring Dads only after intervention for domestic violence) or invitations to service (e.g. all fathers in high conflict divorces) on the basis of any one feature of men’s situation. Instead, we recommend that there be open conversation between Caring Dads and women abuse intervention programs to facilitate easy referral from one to the other and that, in any individual case, the circumstance of men, women and children be assessed and considered to determine the course of intervention.
One consideration is timing. The faster that we can engage high-risk fathers in interventions that involve assessing and monitoring their abusive behaviour in their families the better; so for men who are perpetrating violence against their children and their children’s mothers, referral will sometimes depend on which service they can access first.
A second consideration is accountability. Men are sometime court-ordered to attend a batterer intervention program, and we would never "substitute" Caring Dads for such an order but rather recommend concurrent (in cases of moderate or high risk) or sequential service provision.
A third consideration is the nature of men’s presenting problems and of available referral streams. There are many families identified by child protective services, family courts, child and family mental health and fathering programs where men’s past perpetration of domestic violence is of concern. These men generally do not (and in some cases, cannot) access batterer intervention programs, particularly when men’s abuse has not been physical or included threats to his partners’ safety (i.e., emotional and verbal abuse only). Although for some of these men (i.e., men actively engaged in ongoing women abuse), immediate referral to program addressing woman abuse may be necessary, other men may be able to benefit from Caring Dads without having first completed a program specific to abuse in the intimate relationship. An example is cases where there is a documented history of domestic violence (and an absence of intervention), but where fathers are now the sole caregivers to children and where children’s mothers are not, or minimally, involved with their children.
What are the perspectives of women on Caring Dads?
Given the connection between the safety and well-being of mothers and that of children, it seems critical to understand and incorporate women’s perspectives on Caring Dads and other programs addressing parenting with abusive men. Pioneering programs have been vigilant to this concern, and most have involved women’s advocates as part of program development.
For example, Caring Dads was developed with a community advisory committee that included representatives from shelters, women’s advocacy services, child welfare, family court and child and family mental health services. However, a growing body of research on mothering in the context of domestic violence suggests that "hearing" women’s voices on the value and potential harm of parenting interventions for men who batter is likely to be much more complex.
Battered women face numerous unique challenges in mothering (e.g., Létourneau, Fedick & Willms, 2007; Levendosky & Graham-Bermann, 2001). For example, Lapierre (2010) documented that abused mothers hold an increased sense of responsibility in regards to their children, and do so in the context of fairly significant loss of control over mothering due the impact of DV on women’s physical and mental health, on the disregulation of children’s behaviors and sometimes, due to the multiple and conflicting social services involve in women and children’s lives.
Importantly, Lapierre’s (2010) also documented the centrality of mothering in men’s violence. Women explained that men routinely used mothering as a target in their violence (e.g., by frequently criticizing women for being bad mothers or by using or threatening to use violence against the children as a way to impact women’s parenting). Caring Dads facilitators need to be vigilant to these concerns, monitor and assess them as part of mother contact and, to the extent possible, ensure that men’s participation in Caring Dads does not reduce mothers ability to advocate for safety for her children.
Is caring dads a psycho-educational group or a form of group counselling?
Groups differ enormously in their goals, functioning and organization. In an attempt to standardize understanding of group and to develop reasonable training standards, the Association of Specialists in Group Work (ASGW) delineated major group types, two of which are relevant to understanding Caring Dads: psycho-educational and counseling/interpersonal problem-solving groups. Psycho-educational groups are those designed to give participants relevant information and skills, accompanied by the encouragement of interpersonal discussion and sharing, in order to enhance their understanding, development and decision making so that future problems are prevented. Most parenting groups are psycho-educational in nature. Psycho-educational groups are generally time-limited and focused on specific knowledge and skills-based goals. Focus is generally limited to current problems (rather than issues from the past) and there is limited attention to the transference or counter-transference among members. Individuals skilled in leading psycho-educational groups are those who are knowledgeable about the problem area and skilled in imparting information and skills that match to the groups needs. Good psycho-educational group leaders are also able to mesh dynamics of the group with content so that the groups maintain an interpersonal, rather than a lecture or purely educational tone. Counselling/interpersonal problem-solving groups, in contrast, are designed to help group participants to resolve the unusual, yet often difficult, problems of living through interpersonal support and problem solving. Leaders of counselling groups achieve these goals with the deliberate use of major therapeutic strategies and techniques for problem resolution.
Counselling groups are also distinguished from psycho-educational groups in the attention paid to working appropriately with disruptive group members and with being aware of, and responsive to, interpersonal dynamics within the group. In other words, whereas leaders of psycho-educational groups aim to impart knowledge and skills that their clients can apply, leaders of counselling groups aim to make change in key aspects of their clients’ emotions, thoughts, or behaviors.
Fundamentally, Caring Dads is a counseling/interpersonal problem-solving group – not a psycho-educational group. The overall aim and purpose of Caring Dads is to promote change in level of risk that fathers pose to their children’s safety and well-being. To achieve this change, the program makes deliberate use of motivational enhancement counselling strategies and of cognitive behavioural intervention to identify and counter men’s risk-related automatic cognitions. Caring Dads also make use of education and skills building, as is common in psycho-educational groups; however, even this education is provided with the intent to promote a shift in men’s currently problematic patterns of relating to their children and families. This important distinction informs all aspects of running Caring Dads, from the point of intake until the completion of final reports.
Is there concurrent intervention with mothers and children?
In our experience, women partners of men referred to Caring Dads have very wide ranging needs, a few of whom might benefit from concurrent intervention but many of whom would be better served by existing programs and resources.
Does caring dads do a risk assessment?
We do include an assessment of risk in our intake process. At the onset, it is worth acknowledging that risk assessment is a fairly complicated science and that, to date, there are no risk assessment instruments designed to assess men’s risk of maltreating children. It is also important to note that the vast majority of risk assessments capture static risk, not dynamic risk – in other words, they can tell you something about the overall likelihood of a man’s risk, but not about whether his risk at this moment in time is escalating or decreasing. One response to this lack of information is to take the position that, since we cannot be sure that we are assessing risk accurately, it is best to avoid assessment of risk altogether. Although this may be a reasonable position in the court system, we deem it poor practice clinically. Professionals involved with Caring Dads are working towards improving the safety and well-being of children. They benefit from having knowledge and understanding about what we do know about men’s risk, even if its application is not perfect.
If we allow for imperfect assessment of risk, the next issue of what should be considered as part of risk assessment. There have now been a number of studies of very serious or lethal father-child maltreatment. For example, Cavanagh, Dobash & Dobash (2007) examined data from 26 cases of fatal child abuse perpetrated by fathers, Yampolskaya and Greenbaum (2009) examined characteristics and profiles of 196 male child maltreatment perpetrators in Florida including 126 who committed fatal assaults, and Coohey (2006) identify factors that predicted recidivism among physically abusive fathers. The results of these studies suggest that risk for this population might best be captured by an assessment for domestic violence (such as the SARA which captures risk for general criminality, risks relevant to mental health, and risks specific to intimate partner violence), supplemented with the following indicators:
○ Being a step-father to the child potentially at risk
○ Living common-law with the at-risk child’s mother
○ Child under fathers’ care is under the age of four
○ Evidence of father perpetrating previous incidents of maltreatment against this child or another child in the past
○ Father has injured a child in the past
○ Any prior events where fathers have kept children significantly longer than he was supposed to
Our recommendation to agencies running Caring Dads is to first look to men’s referral agents for level of risk already assessed. Ideally, men will have a risk assessment on file that captures general criminal risk, risk for domestic violence or risk for child maltreatment. Agencies can then supplement that risk assessment with questions on domains not yet covered. How and when this additional information is collected will need to be determined by each agency. Gathering additional information might be part of the intake discussions. Men might provide some of this information via self-report, or some might be gathered from the referral source. We also suggest that individuals across agencies think about the dynamic factors that influence risk for a particular father and child. Hence, it is useful for the referral to speculate on circumstances and conditions likely to increase and decrease risk for this client. Once all the information is collected, it can be used to help guide the level of monitor and the urgency of response necessary for an individual client.
Does Caring Dads teach fathers strategies to change child misbehaviour?
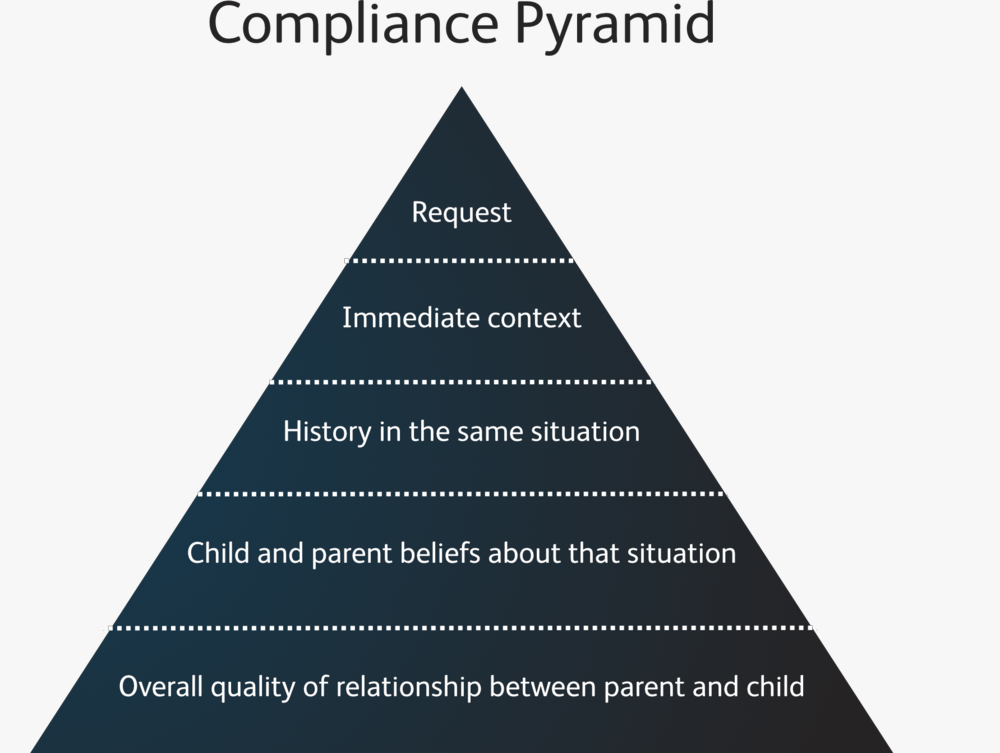
In the Caring Dads program, we do talk with men about child misbehaviour. However, unlike many parenting programs that teach a set of strategies to use when children misbehave, we encourage program participants to think more broadly about their relationship with their children. We do this because we believe that a parent can only be effective in managing child misbehaviour in the longer term if he has developed a strong and healthy emotional connection with his child. It is this relationship that forms the foundation necessary for effective discipline.
The diagram we use to represent this is the "Compliance Pyramid". The pyramid represents the layers and factors that contribute to whether a child does or does not respond to a specific request or instruction in a way that a parent desires. The point of the pyramid analogy is that child compliance is multi-determined and that factors not immediate to the situation have a large role in determining child compliance. In other words, parents need to build up to child compliance layer by layer, starting with a good relationship, moving to positive beliefs, and so on. Even great parenting skills and child management strategies (top layers of pyramid) will not be effective if the bottom of the pyramid is eroded - if the quality of relationship between fathers and their children is poor. For this reason, in Caring Dads, more time is spent building fathers' relationship with their children and exploring their beliefs than on developing immediate solutions for child management challenges.
{kind=link}